Reasons for absenteeism in rural primary schools in two Colombian municipalities
Razones de ausentismo en escuelas primarias rurales de dos municipios colombianos
Razões do não comparecimento nas escolas primarias rurais nos municípios colombianos
Artículos Originales
Recibido: 30/01/2020
Aprobado: 25/02/2020
Publicado: 18/05/2020
Autores
Sandra Lucía Vargas
María Inés Matiz
Víctor Alberto Olano
Diana Sarmiento-Senior
Juan Felipe Jaramillo
Neal Alexander
Audrey Lenhart
Thor Axel Stenström
Hans J. Overgaard
Abstract
Background: School absenteeism is a considerable problem generally related to higher dropout rates, poor academic achievement and school lag. This study determined the frequency and causes of overall and illness-related absenteeism of students in rural schools from two Colombian municipalities.
Methods: A prospective and descriptive study was conducted in a population of 948 school children from 34 rural schools. Absenteeism data were collected for 2013 academic year consisted of the number of students registered and absent by grade, school, day and reason for absence. Absence rates (overall and illness-related absenteeism) were recorded, based on full or partial days absence, measured both as episodes, and accumulating the number of days.
Results: From the students included in the study, 55.1% were male and 71.6% were between 5 and 9 years old. The overall absence rate was 5.7 episodes per child-year (95% confidence interval 5.5 to 5.8) and 8.6 days per child-year (8.4 to 8.9). The main reasons for non-attendance were illness (24.4%), medical or dental check-up (12.9%), travel (12.3%), lack of motivation to attend school (10.0%) and bad weather (9.3%). The illness-related absence rate was 1.4 episodes per child-year (95% confidence interval 1.3 to 1.5) and 2.5 days per child-year (2.4 to 2.6). The main reasons for illness-related absence were cold (37.0%), nonspecific fever (10.9%) and stomach pain or vomiting (8.4%).
Conclusions: In this study, the most common reasons for non-attendance were illness-related. The importance of respiratory and gastrointestinal infections in absenteeism was evident, showing rates similar to other urban school studies. Then, the results of this study provide knowledge on the magnitude and reasons for absenteeism in rural schoolchildren.
Resumen
Antecedentes. El ausentismo escolar es un problema importante relacionado con altas tasas de abandono escolar, bajo rendimiento académico y rezago escolar. Este estudio determinó la frecuencia y las causas del ausentismo general y el ausentismo relacionado con la enfermedad en estudiantes de escuelas rurales de dos municipios de Colombia.
Métodos. Se realizó un estudio descriptivo en una población de 948 escolares de 34 escuelas rurales. Los datos de ausentismo recopilados para el año 2013 consistieron en el número de episodios y días de ausentismo por grado y motivo de ausencia general y por enfermedad. Se calcularon las tasas de ausentismo general y por enfermedad.
Resultados. El 55,1% de la población participante eran hombres y el 71,6% tenían entre 5 y 9 años. La tasa de ausentismo general fue 5,7 episodios por niño-año, IC 95% (5,5-5,8) y 8,6 días por niño-año, IC 95% (8,4-8,9). Las principales razones del ausentismo fueron enfermedades (24,4%), chequeo médico u odontológico (12,9%), viajes (12,3%), falta de motivación para asistir a la escuela (10,0%) y mal clima (9,3%). La tasa de ausentismo por enfermedad fue 1,4 episodios por niño-año IC 95% (1,3-1,5) y 2,5 días por niño-año IC 95% (2,4-2,6). Las principales razones del ausentismo por enfermedad fueron el resfriado común (37,0%), la fiebre inespecífica (10,9%) y el dolor de estómago o vómito (8,4%).
Conclusiones. Las razones más comunes para la no asistencia estuvieron relacionadas con la enfermedad. La importancia de las infecciones respiratorias y gastrointestinales en el absentismo fue evidente, mostrando tasas similares a las de otros estudios en escuelas urbanas. Los resultados de este estudio proporcionan conocimiento sobre la magnitud y las razones del absentismo en la población escolar rural
Resumo
Antecedentes. O absentismo escolar é um grande problema relacionado às altas taxas de evasão escolar, baixo desempenho acadêmico e atraso escolar. Este estudo determinou a frequência e causas do não comparecimento geral e por doenças em estudantes de escolas rurais de dois municípios da Colômbia.
Métodos. Estudo descritivo, realizado em uma população de 948 escolares de 34 escolas rurais. Os dados de absentismo coletados para 2013 consistiram no número de episódios e dias de não comparecimento por grau e motivo da ausência geral e por doença, foram calculadas as taxas de cada evento.
Resultados. 55,1% da população participante eram crianças masculinas do primeiro grau, 71,6% entre 5 e 9 anos de idade. A taxa geral de absentismo foi de 5,7 episódios por criança-ano, IC95% (5,5-5,8) e 8,6 dias por criança-ano, IC95% (8,4-8,9). Os principais motivos do não comparecimento foram doenças (24,4%), check-up médico ou odontológico (12,9%), viagens (12,3%), falta de motivação para frequentar a escola (10,0%) e mau tempo (9,3%). A taxa de absentismo da doença foi de 1,4 episódios por IC95% criança-ano (1,3-1,5) e 2,5 dias por IC95% criança-ano (2,4-2,6). Os principais motivos da ausência de doença foram resfriado comum (37,0%), febre inespecífica (10,9%) e dor de estômago ou vômito (8,4%).
Conclusões. Os motivos mais comuns de não comparecimento foram relacionados à doença. A importância das infecções respiratórias e gastrointestinais no absenteísmo foi evidente, mostrando taxas semelhantes às de outros estudos em escolas urbanas. Os resultados deste estudo fornecem informações sobre a magnitude e as razões para evasão escolar na população escolar rural.
Introduction
Academic success depends largely on student attendance at school. Student absence strongly affects the results of standardized testing, graduation and dropout rates (1). Therefore, student absence is a concern of educational institutions and authorities. Despite many efforts to reduce absence, it remains a complex and challenging problem for the education system (2). Recently, the International Network for School Attendance (INSA) was founded to promote school attendance, reduce absenteeism and solve school attendance problems (3).
In the last 50 years, there have been several studies on school absence in North America and Europe, but few in developing countries. In the United States, there is controversy as to the main causes of school absenteeism, and the importance of socioeconomic factors and educational quality (4). A rural study in India, reported adverse weather conditions, child labor and illness as the main reasons for absenteeism (5). A meta-analytic review revealed significant and substantial effects for school absenteeism related to physical and mental problems of the child, substance abuse, antisocial or risky behavior, problems at or with school (e.g., having a negative school attitude), characteristics of the school (e.g., low quality of the school or education system), parenting and family problems (6).
Schools are frequently affected by outbreaks of infectious, causing increased absenteeism of students and teachers, increased health spending, and decreased learning process among children (7,8). In 2012-2013, approximately 19% of students from preschool to fifth grade in New York City were absent for at least 10% of the academic year (9), a level considered as chronic absenteeism. Similarly, schools in low-income neighborhoods reported chronic absenteeism rates up to 40% (9).
School absenteeism due to health problems is also an important concern of public health authorities. Lau et al (2012) attributed about 75% of all school absences to illness (10). In the United States, 3.5% of school-aged children missed 11 or more days of school in the last year because of illness or injury (11). Infectious diseases are a major reason for absenteeism in students in elementary schools (8). A systematic review of pediatric influenza identified that the average length of absence from school or day care associated with confirmed influenza ranged from 2.8 to 12 days for children (12). In Ohio (USA), a study reported that among the main causes of illness-related absence were gastrointestinal and respiratory infections (13).
Children often do not attend school due to minor illnesses like colds or minor pain. These children often return to the classroom without long-term consequences for their education. However, children with chronic illnesses like asthma, migraine headaches, mental health conditions, and eczema/psoriasis/skin disorders have frequent absences due to medical appointments, therapies, or acute episodes of illness. Recurrent absenteeism due to these illnesses hinders academic progress, increases dropout rates and affects professional career success in adulthood (14-16).
Absenteeism affects the self-esteem and academic performance of children. It affects not only educational attainment, but also interferes with screening programs and interventions by health institutions in schools (5). Moreover, it most often affects the population sectors that suffer marginalization or social or economic deprivation, e.g. ethnic minorities and rural populations. Currently, various longitudinal studies revealed sustained or increasing rates of absenteeism (1,3,17,18).
Education is considered a fundamental right in Colombia. However, there are gaps in coverage and quality, affecting lower income households, specific regions, rural population and ethnic minorities. In 2015, there was a mean of 5.5 years of education in rural while in urban areas was 9.2 years (19,20).
In Colombia, there are just a few studies on school absenteeism, and most of them have been conducted in the urban area. These studies report absenteeism rates around 1.0 day per child-year, with outstanding definition and measurement period differences (21-27). Some of these studies identify family dysfunction and health problems such as asthma and rhinitis as variables that explain higher rates of absenteeism and poor academic performance (25-27). One of the difficulties in describing this problem is the lack of reliable statistics at national and local level, particularly in rural areas.
Then, to gain a greater understanding of the frequency and causes of overall illness-related school absenteeism in rural schools, a study was conducted in the municipalities of Anapoima and La Mesa, two towns located in Cundinamarca, a province in the central region of Colombia, as part of a larger project on school-based dengue and diarrhea control (28).
Metodology
Study area
This study was conducted at 34 rural primary schools from Anapoima and La Mesa, two municipalities from the province of Cundinamarca, Colombia. All participant schools were enrolled on the “Escuela Nueva Model”, a multi-grade classroom.
The municipality of Anapoima has a population of 13,700 inhabitants and La Mesa 30,250 inhabitants, of which 58% and 42% live in rural areas, respectively (29,30). The main sources of income in the two municipalities are agriculture (sugar cane, coffee and fruit), along with tourism (29,30).
All the schoolchildren registered on every rural school of both municipalities in 2013 were included. In Anapoima, 400 children, aged 4-15 years, participated in the study; and in La Mesa, 548 children aged 4-16 years participated also. In 2010, the proportion of people with Unmet Basic Needs (UBN) in the rural areas of Anapoima and La Mesa were 36.4% and 36.8%, respectively (31,32). The UBN index is a direct method to identify critical shortages in a population, mainly to characterize poverty; it is composed of indicators such as housing, sanitation, basic education, and minimum income. In 2013, the dropping out proportion of children in La Mesa was 5.4% and in Anapoima was 2.2 (33). In 2017, both municipalities had higher dropout rates in rural areas, as such: Anapoima 0.5% vs 2% and La Mesa 3% vs 3.6%. Compering with the national dropout rate levels they were 3.7% vs 4.2%, and with the Province of Cundinamarca 3.0% vs 2.9% (34). Data about absenteeism were not found.
Data collection
Absences were recorded daily in a format that included the child's name, date of start and end of absence, reason for absence (illness, bad weather, travel, lack of motivation, other and unknown reason) and who gave the information. ‘Other’ reasons were noted and later categorized. If the reason for absence was illness it was noted whether the student consulted health services, what the diagnosis was (dengue, diarrhea, flu, other, unknown), and what kind of symptoms had (fever, diarrhea, vomiting, headache, cough / runny nose, skin rash, others, unknown). This questionnaire was completed by schoolteachers during the 2013 school year (January 21 to November 22, covering 39 school weeks).
An absence episode was defined as the non-presence of the student throughout all, or part of a school day. For example, a child who got sick while at school and returned home before the end of the school day was recorded as an absence episode. Overall absenteeism was defined as not attending school for any reason, including illness. An absence episode due to illness was defined as non-presence of the student due to any illness or symptoms. Absence for health reasons were established by phone calls to parents and, when parents could not be contacted by phone, house visits were conducted. A new absence episode was defined when at least three days passed without absence for the same reason from the last day of an episode to the new one. The length of an absence episode was specified as the number of days between and including the first and the last day of absence (excluding weekends and holidays). The term chronic absence was used when one student was absent more than 10% of the school year for any reason (1).
In cases where the absence was due to illness or the motive was unknown, a group of project assistants called the parents or guardians of the child to establish the reason. During this phone call questions were asked about the child’s symptoms, including gastrointestinal, respiratory or other symptoms, whether health services were consulted, and history of hospitalization.
A respiratory infection was defined as a subject having at least two of the following symptoms: (a) nasal discharge, (b) stuffy or blocked nose or noisy breathing, (c) cough, (d) feeling of chills or fever (e) throat pain, or (f) sneezing (35). Gastrointestinal infection was defined as one or both of the following: (a) passage of three or more loose or liquid stools (or more frequent passage than is normal for the individual) during a 24 hours’ time period or (b) any episodes of vomiting (35). Probable dengue cases were defined according to WHO criteria (36).
Data analysis
The total number of absence episodes, length in days, the proportion of absences attributable to each cause, rate of absence episodes and rate of absence days in each school were calculated. These rates were expressed per year based on a school year of 185 days and the confidence intervals were calculated performing a Poisson distribution.
Data were entered into Microsoft Excel version 2007 and analyzed in SPSS version 21.
Ethical considerations
The project was presented to school principals and teachers who signed consent to participate on behalf of each school. The study was approved by the Comité Institucional de Ética en Investigaciones de la Universidad El Bosque, Bogotá, Colombia (Acta No. 146 of 30/08/2011) and the Ethical Review Board of London School of Hygiene and Tropical Medicine (Ref. no. 6289). Written consent and acceptance were documented by most parents and involved students. Parental consent was sought via information and consent forms that students were asked to take home. Some forms were mislaid and, comparing the ones already returned, many were found to be illegible, or unidentifiable for other reasons such as names being incomplete or at high variance with those in our records. However, oral consent from parents or guardians was sought as well during telephone calls when establishing reasons for student school absences. Bearing in mind that this study had a minimal risk in terms of the Colombian Ministry of Health, Resolution 8430 of 1993, a permission was sought and received from the ad-hoc ethical committee of the Universidad El Bosque (Acta No. 009 of 27/11/2014) and from the Ethics Committee of the London School of Hygiene and Tropical Medicine (reference 10453/6289, 7 March 2016) to publish all data collected.
Results
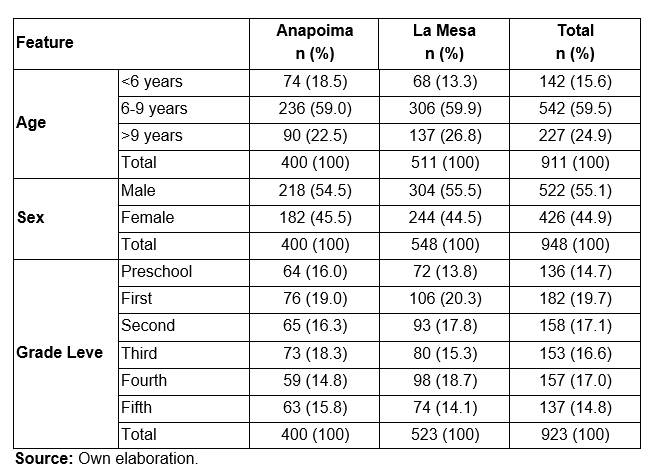
A total of 948 school children and adolescents were included in the study. The characteristics of the study population are shown in Table 1. Data are lacking for 37 children in relation to age and 25 related to grade. The mean age was 7.9 years (range 12). From the total of students that entered the study at the beginning of the school year, 160 (16.9%) withdrew before completing the school year and 184 (19.4%) were enrolled after the school year started.
Overall absenteeism
The total number of absence episodes was 4241. Of these 2377 (56.0%) were in La Mesa and 1864 (44.0%) in Anapoima. A total of 6481 absence days were recorded, 3837 (59.2%) in La Mesa and 2644 (40.8%) in Anapoima. A large proportion (81.1%) of children were absent one or more days during the school year; all the children in two schools in Anapoima and one in La Mesa did not attend at least once a year. Three quarters of the absences lasted for one day.
There was an average of 5.7 absence episodes per child-year (CI95% 5.5-5.8) and 8.6 absence days per child-year (CI95% 8.4-8.9) (Table 2). There were no substantial differences between the two municipalities related to the mean number of absence episodes (Anapoima: 6.5 episodes/student/year; La Mesa: 5.5 episodes/student/year) and number of days (Anapoima: 9.0 days/student/year; La Mesa: 9.5 days/student/year). Chronic absenteeism occurred in 64 (6.8%) students who were from 20 out of the 34 analyzed schools (58.8%).
Table 2. Number and rates (per child-year; 95% confidence interval) and days of absence episodes from 34 schools in rural areas at the municipalities of Anapoima and La Mesa, Cundinamarca, Colombia. 2013.

a Overall absence includes illness-related absence, respiratory infections and gastrointestinal infections.
b Illness-related absence includes respiratory infections, gastrointestinal infections and fever.
Source: Own elaboration.
Overall absenteeism and illness rates were highest among children under 6 years of age and females. Regarding grades, the highest rates of absenteeism were the preschool and the first-grade groups (Table 3).
Table 3. Number and rates (per child-year) of absence episodes and days by sex, age and school grade in 34 schools belong to rural areas at the municipalities of Anapoima and La Mesa, Cundinamarca, Colombia. 2013.

Source: Own elaboration.
Absenteeism reasons
The main reasons for absenteeism were general illness, medical or dental check-up, travel to the urban area of the municipality or another city, lack of motivation to go to school and adverse weather conditions, making travel to school very difficult. The study design did not distinguish whether medical and dental check-ups were made for sick or healthy children. The main reasons for absenteeism are shown in Figure 1.
 Figure 1. Percentage of the reason of overall absence episodes in students from 34 rural schools.
Figure 1. Percentage of the reason of overall absence episodes in students from 34 rural schools.
*Moreover, other reasons included were distance to school, lack of money for transportation, lack of escort to go with the child to the school, bereavement or other family misfortune, overslept, stayed at grandparents, moved to another house, religious festivities, unknown of scheduled classes, adaptation to school issues (for very small children).
Source: Own elaboration.
Absenteeism due to illness
The total number of absence episodes due to illness was 1025 distributed almost equally between municipalities (La Mesa: 1.1 episodes, 2.4 days/student/year and Anapoima: 1.8 episodes, 3.0 days/student/year). The total number of absence days was 1864 (Table 2). Almost half (49.1%) of the students were absent due to illness for one or more days during the school year and 67.5 % of the episodes lasted one day. The range of duration of illness-related absence episodes was 1 to 33 days.
The highest rates of illness-related absenteeism were due to respiratory infections, gastrointestinal infections and fever of unknown origin (Table 2).
The main reasons for absenteeism from respiratory infectious were common cold, tonsillitis, ear pain, ear infections and asthma. Due to gastrointestinal infections, the main reasons were stomach pain, vomiting, diarrhea and indigestion. Also, other important reasons for absenteeism due to illness were injuries, headache, dental problems and dengue (Table 4).
Table 4. Absenteeism due to illness in students from 34 schools in rural areas at the municipalities of Anapoima and La Mesa, Cundinamarca, Colombia. 2013

The illnesses that caused the longest absence episodes were chicken pox (average 5.9 days), dengue (average 4.0 days), and pharyngitis (average 2.2 days).
Fever was reported in 541 episodes, associated with 1,031 absence days. The distribution of illness episodes reporting fever were cold 53%, nonspecific fever 20.3%, pharyngitis 6.5%, diarrhea 6.3% and dengue 3.5%.
The largest number of illness episodes occurred in August. Common cold and dengue were most common in June, but diarrhea, stomach pain and vomiting had a greater number of episodes in October.
Ten students (1.1%) were absent from school for ten or more days due to illness. These children were absent from 1-10 times in the school year. One student was absent once for 33 days because of surgery. Some students had a longer episode of school absence, for example hepatitis (16 days), dengue (13 days), measles (12 days), chicken pox (12 days), flu (11 days), injuries (10 days), asthma (9 days) and trauma (7 days).
The total number of kids with absences related to asthma was 18 (1.9%). Students reporting asthma-related absence were absent from school three times more, compared to those with other illnesses, with 3.7 vs. 1.3 episodes per student/year and 7.8 vs. 2.4 days per student/year, respectively.
Discussion
School absenteeism was carried out in students aged 4-16 years throughout the 2013 school year at 34 rural schools in two municipalities from Colombia. The most common reasons for absence were illness (24.4%), medical or dental check-ups (12.9%), traveling (12.3%), lack of motivation to go to school (10.0%), and bad weather (9.3%). In Latin America, school absenteeism is generally related to poverty, for example inability to cover school expenses and transport to the school, particularly in rural areas (3,37). In this study these reasons only corresponded to 2.1%. Previous data from Colombia suggested that the main reasons for school absence were lack of resources, the need to work, lack of interest in school, and adverse conditions, hindering access to rural schools (38).
Some studies show that other reasons for absence in school are health problems, malnutrition and child labor (37). A recent study conducted in these municipalities found an association between higher rates of school absenteeism and stunting or low height by age (39). The lack of interest of the parents of the children for education, the lack of support and attention by the teachers and insufficient attendance supervision and performance of the students were also reported reasons for school absence (37). Some of these motives were among the main reasons for school absenteeism found in our study, e.g. the lack of motivation to go to school was 10.0%.
The limited gains in academic performance of schools in rural areas have been the subject of several studies and the conclusions were, in general, that these difficulties resulted from the socioeconomic conditions as well as the nature of the educational system in rural areas. In these mentioned areas, there is a pedagogical-didactic structure based on heterogeneity and a multilevel group of different ages tangle with organizational and administrative singular structure (3,40-44). Huge aspects that should be pointed out in these two municipalities, considering that lack of motivation was the fourth most common cause of school absenteeism, bad weather hampering access was the fifth, and children’s work and domestic tasks were among the ten main reasons. These causes of absenteeism reflect the disadvantages of children and adolescents in rural areas, since 70% of parents or caregivers in these municipalities have not completed primary education, in addition to having poor schools infrastructure; as it has also been reported in similar studies in the United States, Latin America and Colombia (9,45-47).
Illness was the leading cause of school absenteeism. In this study, the students lost an average of 2.5 days per academic year due to sickness. However, the magnitude of absence due to illness could be underestimated because absences due to a medical or dental appointment did not distinguish between illness and routine checkups.
Absenteeism from infections is one of the major problems in public and private schools (48). In the current study, respiratory and gastrointestinal infections were the most common reasons for illness-related absence, similar to those reported in other studies (49,50). The impact of respiratory and gastrointestinal infections on illness-related absenteeism was evident, causing about a third of the lost days.
The incidence of major infectious diseases such as dengue and influenza are higher in primary than in secondary schools (51,52). Although dengue is endemic in the study area, and 2013 was an epidemic year (53), absence due to dengue was only 2%; even so, nonspecific fever was the second reason for illness-related absence, and some of such episodes could have been related to dengue. Health services were consulted in only 27.5% of the illness absences. The use of absence data could be a useful strategy for surveillance and outbreak detection (54), taking into account the barriers to access health services in rural areas (55).
Risk of gastrointestinal infections is heightened in Colombia by poor access to clean water, sanitation and hygiene, since only 54% of rural public schools have access to potable water, 57% to sewerage, and only 40% have enough bathrooms (56). Intestinal parasites and other pathogens could be an important health issue for research in these two municipalities because of diarrhea, vomiting and stomach pain were the third and fourth most common causes of illness-related absenteeism. In Peru, high morbidity due to parasitic infections had a direct effect on school absenteeism (57).
The main causes of chronic absenteeism due to illness in the current study was similar to other studies in the US and other countries (15,27). Children with special needs, for example asthma, can have rates of absenteeism up 50% higher than average, contributing to poor academic achievement and higher dropout rates (14,26).
Chronic dental problems can also affect school attendance (58). In our study, only 3.3% of absences were due to dental problems, much less than the 22.5% reported in a study in Thailand (59). However, this issue might be underreported in our study, because when students went for a dental appointment it was not clear whether they went for a dental check-up or illness. More research is required to explore the relationship between absenteeism for dental reasons and severity of the dental conditions. Furthermore, in Colombia, other studies have shown that children in rural areas have worse oral health indicators than children in urban areas, suggesting greater inequity and poor access to health care (60).
As mentioned in the Mission for Transformation of the Country Report, Colombia has a historic debt with the rural area (61). The first point of The Havana Peace Agreement suggests a Comprehensive Rural Development. In education, it proposes to design a Rural Education Special Plan that makes possible for young people to stay in the country areas while doing productive task, allowing also the educational institutes to make important contributions in rural development (61). Thus, educational institutes in rural areas of Colombia shows the big challenges for the post-conflict era, becoming a vital factor to close the huge urban-rural gap.
Absenteeism and dropping out of the school become a multifactorial issue, being the social, economic, family and school the most important, which make it difficult to cover from an exclusive school factor. Moreover, characteristics of rural areas such as lower number of students by grade, long distances between settlements or child labor during harvest seasons are complex problems and require creative solutions. Other important factor is the fact that rural education rarely establish links with productive projects and does not develop work programs along with an effective articulation with technical and technological education (61).
School absenteeism is an initial symptom before dropping out happens. Therefore, it is important to monitor assistance dynamics to intervene early. Absenteeism can raise prejudice over students affected, their families and, in general, society, limiting rights to a comprehensive development of children and adolescents.
In conclusion, this study contributes to knowledge about school absence — overall and due to illness— in schoolchildren of Colombian´s rural areas. In this country, few previous studies of absenteeism emphasized dropout rates and did not evaluate absenteeism as dropping out signal. It is also important to consider the impact of infectious diseases on school attendance, considering the conditions in rural areas in terms of access to health services, limitations of school health surveillance systems, and poor water, sanitation and hygiene, among others.
In addition, the need of improving systems to record school absenteeism could be a useful tool for strengthening illness surveillance systems in these areas. It is important to know the health-related causes of school absenteeism and establish whether there is a relationship with the frequency of illness at the community level. The formulation of effective policies and action plans to reduce absenteeism requires the collaboration among health professionals, local authorities and the education community to reach intervention on social determinants and control of the main causes. Then, the results of this study encourage existing intersectoral collaborations to strengthen and establish new multidisciplinary partnerships to learn in depth about the relationship between student absenteeism and school permanence.
One limitation of this study was that illness diagnosis is based on symptoms reported by parents or guardians without microbiological confirmation and details of health care professionals. The comparison of our data with other studies is limited by large variation in evaluating school absenteeism methodology, since there is no standardized tool that can be applied worldwide.
Conflict of interest
The authors report no conflicts of interest.
Funding
This project was funded by the Research Council of Norway as part of HEALTHPLATFORM study (Grant ref. No 201349), the Lazos de Calandaima Foundation, and the Universidad El Bosque.
Acknowledgements
We thank the mayors, health departments and staff education and rural schools in these municipalities for their cooperation during this project, as well as the following field workers: Humberto Mosquera, Nancy Herrera, Rosa Silva, Laura Cabezas, Paola Moreno, Sandra Moreno, Esmeralda González, Rosa Pulido and Luz Marina Contreras.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of any sponsoring entities.
References
- 1. Balfanz R, Byrnes V. The importance of being in school: A report on absenteeism in the nation's public schools. Baltimore: Johns Hopkins University Center for Social Organization of Schools; 2012.
- 2. García-Grácia M. Culturas de enseñanza y absentismo escolar en la enseñanza secundaria obligatoria: estudio de casos en la ciudad de Barcelona. Revista de Educación 2005;(338):347-76.
- 3. Heyne D, Gentle-Genitty C, Landell MG, Melvin G, Chu B, Gallé-Tessonneau M, et al. Improving school attendance by enhancing communication among stakeholders: establishment of the International Network for School Attendance (INSA). Eur Child Adolesc Psychiatry. 2019:1-8. DOI: 10.1007/s00787-019-01380-y.
- 4. Reid K. The causes, views and traits of school absenteeism and truancy: An analytical review. Research in Education 2005;74(1). DOI: 10.7227/RIE.74.6.
- 5. Ananthakrishnan S, Nalini P. School absenteeism in a rural area in Tamilnadu. Indian Pediatrics. 2002;39(9):847-50.
- 6. Gubbels J, van der Put CE, Assink M. Risk factors for school absenteeism and dropout: a meta-analytic review. J Youth Adolesc. 2019;48(9):1637-67. DOI: 10.1007/s10964-019-01072-5.
- 7. McKenzie JE, Priest P, Audas R, Poore MR, Brunton CR, Reeves LM. Hand sanitisers for reducing illness absences in primary school children in New Zealand: a cluster randomised controlled trial study protocol. Trials. 2010;11(1):7. DOI: 10.1186/1745-6215-11-7.
- 8. Dyer DL, Shinder A, Shinder F. Alcohol-free instant hand sanitizer reduces elementary school illness absenteeism. Fam Med. 2000;32(9):633-8.
- 9. Nauer K, Mader N, Robinson G, Jacobs T, Cory B, Moss J, et al. A better picture of poverty. What chronic absenteeism and risk load reveal about NYC’s lowest-income elementary schools. New York: Center for New York City Affairs, The Milano School of international affairs, management, and urban policy; 2014 [cited 2019 Aug 28]. Available from: https://www.attendanceworks.org/wp-content/uploads/2017/06/BetterPictureofPoverty_PA_FINAL_001.pdf
- 10. Lau CH, Springston EE, Sohn MW, Mason I, Gadola E, Damitz M, et al. Hand hygiene instruction decreases illness-related absenteeism in elementary schools: a prospective cohort study. BMC pediatrics. 2012;12:52. DOI: 10.1186/1471-2431-12-52.
- 11. Centers for Disease Control (CDC). Life Stages and Populations, Child Health. CDC; 2017 [cited 2019 Aug 28]. Available from: http://www.cdc.gov/nchs/fastats/child-health.htm.
- 12. Antonova EN, Rycroft CE, Ambrose CS, Heikkinen T, Principi N. Burden of paediatric influenza in Western Europe: a systematic review. BMC Public Health. 2012;12(1):968. DOI: 10.1186/1471-2458-12-968.
- 13. Sandora TJ, Shih MC, Goldmann DA. Reducing absenteeism from gastrointestinal and respiratory illness in elementary school students: a randomized, controlled trial of an infection-control intervention. Pediatrics. 2008;121(6):e1555-62. DOI: 10.1542/peds.2007-2597.
- 14. Reeves S, Filce HG. " Splinter Skills” Do not make students sharper! Meeting the needs of elementary students with chronic illnesses and absenteeism. The Delta Kappa Gamma Bulletin. 2012;78(2):57-62.
- 15. Krenitsky-Korn S. High school students with asthma: attitudes about school health, absenteeism, and its impact on academic achievement. Pediatr Nurs. 2011;37(2):61-8.
- 16. Carter-Pokras OD, Bugbee BA, Gold RS, Lauver PE, Aiken R, Arria AM. Utilizing Student Health and Academic Data: A County-Level Demonstration Project. Health Promot Pract. 2019;1524839919862796. DOI: 10.1177/1524839919862796.
- 17. Beach MG. Kindergarten teachers' perceptions of factors related to academic achievement for rural children living in poverty. Ann Arbor: North Dakota State University; 2009.
- 18. Ready DD. Socioeconomic disadvantage, school attendance, and early cognitive development: The differential effects of school exposure. Sociology of Education. 2010;83(4):271-86. DOI: 10.1177/0038040710383520.
- 19. Colombia. Ministerio de Educación (Minsedicación). Plan Nacional Decenal de Educación 2016–2026. El camino hacia la calidad y la equidad. Bogotá D.C.: Mineducación; 2017 [cited 2020 Jan 20]. Available from: http://www.plandecenal.edu.co/cms/media/herramientas/PNDE%20FINAL_ISBN%20web.pdf.
- 20. Delgado-Barrera M. La educación básica y media en Colombia: retos en equidad y calidad. Informe final. Bogotá D.C.: Fedesarrollo; 2014 [cited 2020 Jan 20]. Available from: https://www.repository.fedesarrollo.org.co/handle/11445/190. .
- 21. López-Quintero C, Freeman P, Neumark Y. Hand washing among school children in Bogotá, Colombia. Am J Public Health. 2009;99(1):94-101. DOI: 10.2105/AJPH.2007.129759.
- 22. Arsenault JE, Mora-Plazas M, Forero Y, López-Arana S, Marín C, Baylin A, et al. Provision of a school snack is associated with vitamin B-12 status, linear growth, and morbidity in children from Bogotá, Colombia. J Nutr. 2009;139(9):1744-50. DOI: 10.3945/jn.109.108662.
- 23. Boeke CE, Mora-Plazas M, Forero Y, Villamor E. Intestinal protozoan infections in relation to nutritional status and gastrointestinal morbidity in Colombian school children. J Trop Pediatr. 2010;56(5):299-306. DOI: 10.1093/tropej/fmp136.
- 24. Dennis RJ, Caraballo L, García E, Rojas MX, Rondon MA, Pérez A, et al. Prevalence of asthma and other allergic conditions in Colombia 2009-2010: a cross-sectional study. BMC Pulmonary Medicine. 2012; 12:17. DOI: /10.1186/1471-2466-12-17.
- 25. Paternina-González DH, Pereira-Peñate MM. Funcionalidad familiar en escolares con comportamientos de riesgo psicosocial en una institución educativa de Sincelejo (Colombia). Salud Uninorte. 2017;33(3):429-37.
- 26. Sánchez J, Estarita J, Salemi C. Efecto de la rinitis y el asma en el ausentismo y rendimiento laboral y escolar en una población del trópico latinoamericano. Revista Alergia México. 2016;63(1):32-40. DOI: 10.29262/ram.v63i1.132.
- 27. Enriquez-Guerrero CL, Seguro-Cardona ÁM, Tovar-Cuevas JR. Factores de riesgo asociados a bajo rendimiento académico en escolares de Bogotá. Investig Andina. 2013;15(26):654-66.
- 28. Overgaard HJ, Alexander N, Matiz MI, Jaramillo JF, Olano VA, Vargas S, et al. Diarrhea and controlling dengue in rural primary schools in Colombia: study protocol for a randomized controlled trial. Trials. 2012;13(1):182. DOI: 10.1186/1745-6215-13-182.
- 29. Alcaldía de Anapoima. [cited 2019 Aug 28]. Available from: http://www.anapoima-cundinamarca.gov.co/MiMunicipio/Paginas/Presentacion.aspx.
- 30. Alcaldía Municipal de La Mesa. [cited 2019 Aug 28]. Available from: http://www.lamesa-cundinamarca.gov.co/MiMunicipio/Paginas/Informacion-del-Municipio-.aspx.
- 31. Colombia. Departamento Nacional de Estadística (DANE). Boletín censo general 2005.Perfil municipal Anapoima, Cundinamarca. Bogotá D.C.: DANE; 2010 [cited 2019 Aug 28]. Available from: http://www.dane.gov.co/files/censo2005/PERFIL_PDF_CG2005/25035T7T000.PDF.
- 32. Colombia. Departamento Nacional de Estadística (DANE). Boletín censo general 2005. Perfil municipal La Mesa, Cundinamarca. Bogotá D.C.; DANE; 2010 [cited 2019 Aug 28]. Available from: https://www.dane.gov.co/files/censo2005/PERFIL_PDF_CG2005/25386T7T000.PDF.
- 33. Colombia. Tecnologías de la Información y las Comunicaciones (MinTic). Estadísticas en Educación Básica por departamento. Bogotá D.C.: MinTic; 2020 [cited 2020 Jan 20]. Available from: https://www.datos.gov.co/Educaci-n/ESTADISTICAS-EN-EDUCACION-BASICA-POR-DEPARTAMENTO/ji8i-4anb.
- 34. Colombia. Departamento Nacional de Estadística (DANE). Educación formal: Bogotá D.C.: DANE; 2020 [cited 2020 Jan 20]. Available from: https://www.dane.gov.co/index.php/estadisticas-por-tema/educacion/poblacion-escolarizada/educacion-formal#informacion-2018-por-departamento.
- 35. Lee GM, Salomon JA, Friedman JF, Hibberd PL, Ross-Degnan D, E Zasloff, et al. Illness transmission in the home: a possible role for Alcohol-based hand gels. Pediatrics. 2005;115(4):852-60. DOI: 10.1542/peds.2004-0856.
- 36. World Health Organization (WHO). Dengue guidelines for diagnosis, treatment, prevention and control; new edition. Geneva: WHO; 2009.
- 37. Frankema E. Comparing the distribution of education across the developing world, 1960-2005: What does the grade enrollment distribution tell about Latin America? Social Indicators Research 2008;88(3):437-55. DOI: 10.1007/s11205-007-9213-4.
- 38. Sarmiento-Gómez A, Tovar L, Alam C. Educación, Compromiso de todos, Situación de la educación básica, media y superior en Colombia. Bogotá D.C.: Casa Editorial El Tiempo, Fundación Corona, Fundación Antonio Restrepo Barco y UNICEF; 2001.
- 39. Rodríguez-Escobar G, Vargas-Cruz SL, Ibáñez-Pinilla E, Matiz-Salazar MI, Jögen-Overgaard H. Relación entre el estado nutricional y el ausentismo escolar en estudiantes de escuelas rurales. Rev. salud pública. 2015;17(6):861-73. DOI: 10.15446/rsap.v17n6.48709.
- 40. Sepúlveda.Ruiz MP, Gallardo-Gil M. La escuela rural en la sociedad globalizada: nuevos caminos para una realidad silenciada. Profesorado: Revista del currículum y formación del profesorado. 2011;5(2):141-53.
- 41. Espíndola E, León A. La deserción escolar en América Latina: Un tema prioritario para la agenda regional. Revista Iberoamericana de educación. 2002;(30)3:39-62. DOI: 10.35362/rie300941.
- 42. Clemens MA. The long walk to school: International education goals in historical perspective. SSRN Electronic Journal. 2004;(37). DOI: 10.2139/ssrn.549482.
- 43. Bonal X. On global absences: Reflections on the failings in the education and poverty relationship in Latin America. International Journal of Educational Development. 2007;27(1),86-100. DOI: 10.1016/j.ijedudev.2006.05.003.
- 44. Birdsall N, Ross D, Sabot R. Education, growth and inequality. In: Birdsall N, Jaspersen F, editors. Pathways to growth. Comparing East Asia and Latin America. Washington D.C.: Inter-American Development Bank. 1997. p. 93-130.
- 45. Follman DK. Elementary teachers' perceptions of practices to increase the academic achievement of economically disadvantaged rural students in high poverty schools. Ann Arbor: North Dakota State University; 2011.
- 46. Pardo R, Sorzano O. Determinantes de la asistencia y de la deserción escolar en primaria y secundaria. Bogotá D.C. Panamericana; 2004.
- 47. Frankema E, Bolt J. Measuring and analysing educational inequality: the distribution of grade enrolment rates in Latin America and Sub-Saharan Africa. Groningen: University of Groningen; 2006.
- 48. Colombia. Contraloría General de la Nación. La deserción escolar en la educación básica y media. Bogotá D.C.: Contraloría General de la Nación; 2003.
- 49. Neuzil KM, Hohlbein C, Zhu Y. Illness among schoolchildren during influenza season: effect on school absenteeism, parental absenteeism from work, and secondary illness in families. Arch Pediatr Adolesc Med. 2002;156(10):986-91. DOI: 10.1001/archpedi.156.10.986.
- 50. Dekker LH, Mora-Plazas M, Marin C, Baylin A, Villamor E. Stunting Associated with poor socioeconomic status and maternal nutrition and respiratory morbidity in Colombian schoolchildren. Food Nutr Bull. 2010;31(2):242-50. DOI: 10.1177/156482651003100207.
- 51. Hoen AG, Buckeridge DL, Chan EH, Freifeld CC, Keller M, Charland K, et al. Characteristics of US public schools with reported cases of novel influenza A (H1N1). Int J Infect Dis. 2010;14(Suppl 3):e6-8. DOI: 10.1016/j.ijid.2009.11.034.
- 52. Restrepo BN, Piedrahita LD, Agudelo IY, Parra-Henao, Osorio JE. Frequency and clinical features of dengue infection in cohort schoolchildren from Medellin, Colombia. J Trop Med. 2012;2012:120496. DOI: 10.1155/2012/120496.
- 53. Colombia. Instituto Nacional de Salud (INS). Informe del evento dengue año 2013. Bogotá D.C.; INS; 2013 [cited 2010 Aug 28]. Available from: http://www.ins.gov.co/buscador-eventos/Informesdeevento/Dengue%202013.pdf.
- 54. Lawpoolsri S, Khamsiriwatchara A, Liulark W, Taweeseneepitch K, Sangvichean A, Thongprarong W, et al. Real-time monitoring of school absenteeism to enhance disease surveillance: A pilot study of a mobile electronic reporting system. JMIR MHealth UHealth. 2014;12(2):e22. DOI: 10.2196/mhealth.3114.
- 55. Vargas-Lorenzo I, Vázquez-Navarrete ML, Mogollon-Pérez AS. Acceso a la atención en salud en Colombia. Rev. salud pública 2010;12(5):701-12.
- 56. Duarte J, Gargiulo C, Moreno M. School infrastructure and learning in the Latin American basic education: An analysis from SERCE. Inter-American Development Bank; 2011 [cited 2019 Aug 28]. Available from: https://publications.iadb.org/handle/11319/5449.
- 57. Thériault FL, Maheu-Giroux M, Blouin B, Casapia M, Gyorkos TW. Effects of a post-deworming health hygiene education intervention on absenteeism in school-age children of the Peruvian Amazon. PLoS Negl Trop Dis. 2014;8(8):e3007. DOI: 10.1371/journal.pntd.0003007.
- 58. Jackson SL, Vann WF Jr., Kotch JB, Pahel BT, Lee JY. Impact of poor oral health on children's school attendance and performance. Am J Public Health 2011;101(10):1900-6. DOI: 10.2105/AJPH.2010.200915.
- 59. Pongpichit B, Sheiham A, Pikhart H, Tsakos G. Time absent from school due to dental conditions and dental care in Thai schoolchildren. J Public Health Dent. 2008;68(2):76-81. DOI: 10.1111/j.1752-7325.2007.00051.x.
- 60. Agudelo-Suarez AA, Martínez-Herrera E. La salud bucal colectiva y el contexto colombiano: un análisis crítico. Rev. Gerenc. Polit. Salud. 2009;8(16):91-105.
- 61. Martínez-Restrepo S, Pertuz MC, Ramírez JM. La situación de la educación rural en Colombia, los desafíos del posconflicto y la transformación del campo. Bogotá D.C.: Alianza Compartir-Fedesarrollo; 2016 [citado 2020 Jan 20]. Available from: https://www.compartirpalabramaestra.org/documentos/fedesarrollo_compartir/la-situacion-de-la-educacion-rural-en-colombia-los-desafios-del-posconflicto-y-la-trasformacion-del-campo.pdf.